Bilateral Hallux Valgus Interphalangeus
Overview
 The term "hallux valgus" or "hallux abducto-valgus" are the most commonly used medical terms associated with a bunion anomaly, where "hallux" refers to the great toe, "valgus" refers to the abnormal angulation of the great toe commonly associated with bunion anomalies, and "abductus/-o" refers to the abnormal drifting or inward leaning of the great toe towards the second toe, which is also commonly associated with bunions. It is important to state that "hallux abducto" refers to the motion the great toe moves away from the body's midline. Deformities of the lower extremity are usually named in accordance to the body's midline, or the line bisecting the body longitudinally into two halves. In more severe cases, the hallux continuing in the abductus fashion eventually either overlaps or underlaps subsequent lesser (small) toes especially the second (adjacent toe).
The term "hallux valgus" or "hallux abducto-valgus" are the most commonly used medical terms associated with a bunion anomaly, where "hallux" refers to the great toe, "valgus" refers to the abnormal angulation of the great toe commonly associated with bunion anomalies, and "abductus/-o" refers to the abnormal drifting or inward leaning of the great toe towards the second toe, which is also commonly associated with bunions. It is important to state that "hallux abducto" refers to the motion the great toe moves away from the body's midline. Deformities of the lower extremity are usually named in accordance to the body's midline, or the line bisecting the body longitudinally into two halves. In more severe cases, the hallux continuing in the abductus fashion eventually either overlaps or underlaps subsequent lesser (small) toes especially the second (adjacent toe).
Causes
A bunion is more common in women than men due to women wearing tighter fitting shoes. This condition can cause a variety of different soft tissue and bony complaints which may result in severe pain.
Symptoms
Pain or soreness. Inflamattion and redness. A burning sensation. Numbness on the side of the great toe. Other conditions which may occur secondary to bunions include calluses on the big toe, sore between the toes, ingrown toenails, and stiffness of the joint where the great toe attaches to the foot.
Diagnosis
Clinical findings are usually specific. Acute circumferential intense pain, warmth, swelling, and redness suggest gouty arthritis (see Gout) or infectious arthritis (see Acute Infectious Arthritis), sometimes mandating examination of synovial fluid. If multiple joints are affected, gout or another systemic rheumatic disease should be considered. If clinical diagnosis of osteoarthritic synovitis is equivocal, x-rays are taken. Suggestive findings include joint space narrowing and bony spurs extending from the metatarsal head or sometimes from the base of the proximal phalanx. Periarticular erosions (Martel sign) seen on imaging studies suggest gout.
Non Surgical Treatment
If overpronation is diagnosed early enough, the mechanics of the feet can be adjusted using a prescription orthotic. If orthotics are worn consistently, many major foot deformities can be avoided such as bunions. Early detection is of paramount importance. When a bunion progresses and cannot be controlled by an orthotic, surgical correction may be a consideration. Many advances in bunion correction allow for surgical intervention to make healing and return to normal activities much easier than use of traditional bunion surgery. 
Surgical Treatment
As mentioned above, with mild cases, the bone is cut close to the big toe joint and shifted over into a correct position. The cut bone is held in placed with one or two surgical screws. With this procedure, just the top of the bone is moved over and the bottom of the bone remains in the same place. This technique is called the Austin bunionectomy and refers to type of bone cut that will be made by the Surgeon. There is, however, a limit on how far one can move the bone over with this technique. Its is generally thought that the cut bone should only be moved over a distance equal to half the width of the bone. In somes the bone may be moved over further.
Prevention
Shop for shoes that possess a removable liner, or insole, and stand on the liner after you have removed it from your shoe. This is an effective method to see if your shoe is wide enough in the forefoot to accommodate your bunion. If your bunion and forefoot are wider than the insole, your shoe will squeeze and constrict your bunion and create the symptoms that define this health problem. The insole should also be wide enough to fully accommodate your big toe when it points outward, away from your other toes.
Over-Pronation Cause
Overview
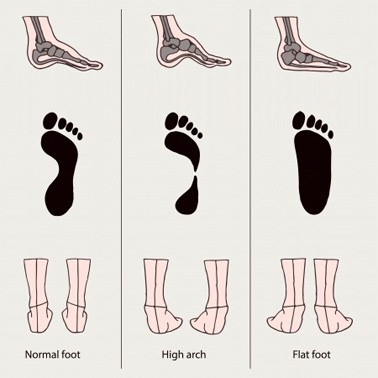
Overpronation is the most common abnormality found in the foot, and for this reason, is the most studied. The term that most people attribute to overpronation is ?flat feet.? Pronation is the rolling in of the foot and the collapse of the arch. Every person pronates to some extent and this is a necessary moment in the normal walking cycle as it allows the forefoot to make complete contact with the ground. Overpronation is when a person pronates too much and for too long. This places excess stress on the tendons and ligaments in the foot and ankle.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.
Non Surgical Treatment
One of the best forms of treatment for over pronation is wearing supportive shoes. Shoes should have ample support and cushioning, particularly through the heel and arch of the foot. Without proper shoes, there may be additional strain on the tissue in the foot, greatly contributing to or causing an occurrence of over pronation. Rarely is surgery considered to relieve the pain and damage that may have resulted from this condition. Orthotic shoe inserts are often the easiest and most effective way to correct pronation.
Prevention
Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise.
Calf stretch:Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times.
Golf ball:While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds.
Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions.
Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times.
Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Overpronation is the most common abnormality found in the foot, and for this reason, is the most studied. The term that most people attribute to overpronation is ?flat feet.? Pronation is the rolling in of the foot and the collapse of the arch. Every person pronates to some extent and this is a necessary moment in the normal walking cycle as it allows the forefoot to make complete contact with the ground. Overpronation is when a person pronates too much and for too long. This places excess stress on the tendons and ligaments in the foot and ankle.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.
Non Surgical Treatment
One of the best forms of treatment for over pronation is wearing supportive shoes. Shoes should have ample support and cushioning, particularly through the heel and arch of the foot. Without proper shoes, there may be additional strain on the tissue in the foot, greatly contributing to or causing an occurrence of over pronation. Rarely is surgery considered to relieve the pain and damage that may have resulted from this condition. Orthotic shoe inserts are often the easiest and most effective way to correct pronation.
Prevention
Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise.
Calf stretch:Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times.
Golf ball:While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds.
Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions.
Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times.
Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Calcaneal Apophysitis The Facts
Overview
Although the name might sound pretty frightening, Sever's disease is really a common heel injury that occurs in kids. It can be painful, but is only temporary and has no long-term effects. Sever's disease, also called calcaneal apophysitis, is a painful bone disorder that results from inflammation (swelling) of the growth plate in the heel. A growth plate, also called an epiphyseal plate, is an area at the end of a developing bone where cartilage cells change over time into bone cells. As this occurs, the growth plates expand and unite, which is how bones grow. Sever's disease is a common cause of heel pain in growing kids, especially those who are physically active. It usually occurs during the growth spurt of adolescence, the approximately 2-year period in early puberty when kids grow most rapidly. This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys. Sever's disease rarely occurs in older teens because the back of the heel usually finishes growing by the age of 15, when the growth plate hardens and the growing bones fuse together into mature bone. Sever's disease is similar to Osgood-Schlatter disease, a condition that affects the bones in the knees.
Causes
Sever?s is often present at a time of rapid growth in adolescent athletic children. At this time the muscles and tendons become tighter as the bones become larger. Between 8 - 15 years of age is the usual onset of this condition.
Symptoms
Symptoms of calcaneal apophysitis may include pain in the back or bottom of the heel, Limping, walking on toes, difficulty running, jumping, or participating in usual activities or sports. Pain when the sides of the heel are squeezed.
Diagnosis
The x-ray appearance usually shows the apophysis to be divided into multiple parts. Sometimes a series of small fragments is noted. Asymptomatic heels may also show x-ray findings of resporption, fragmentation and increased density. But they occur much less often in the normal foot. Pulling or ?traction? of the Achilles tendon on the unossified growth plate is a likely contributing factor to Sever?s disease. Excessive pronation and a tight Achilles and limited dorsiflexion may also contribute to the development of this condition.
Non Surgical Treatment
Cold packs: Apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking.
Shoe inserts: Small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term.
Medication: Pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor).
Anti-inflammatory creams: Also an effective management tool.
Splinting or casting: In severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare.
Time: Generally the pain will ease in one to two weeks, although there may be flare-ups from time to time.
Correction of any biomechanical issues: A physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition.
Education: Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Although the name might sound pretty frightening, Sever's disease is really a common heel injury that occurs in kids. It can be painful, but is only temporary and has no long-term effects. Sever's disease, also called calcaneal apophysitis, is a painful bone disorder that results from inflammation (swelling) of the growth plate in the heel. A growth plate, also called an epiphyseal plate, is an area at the end of a developing bone where cartilage cells change over time into bone cells. As this occurs, the growth plates expand and unite, which is how bones grow. Sever's disease is a common cause of heel pain in growing kids, especially those who are physically active. It usually occurs during the growth spurt of adolescence, the approximately 2-year period in early puberty when kids grow most rapidly. This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys. Sever's disease rarely occurs in older teens because the back of the heel usually finishes growing by the age of 15, when the growth plate hardens and the growing bones fuse together into mature bone. Sever's disease is similar to Osgood-Schlatter disease, a condition that affects the bones in the knees.
Causes
Sever?s is often present at a time of rapid growth in adolescent athletic children. At this time the muscles and tendons become tighter as the bones become larger. Between 8 - 15 years of age is the usual onset of this condition.
Symptoms
Symptoms of calcaneal apophysitis may include pain in the back or bottom of the heel, Limping, walking on toes, difficulty running, jumping, or participating in usual activities or sports. Pain when the sides of the heel are squeezed.
Diagnosis
The x-ray appearance usually shows the apophysis to be divided into multiple parts. Sometimes a series of small fragments is noted. Asymptomatic heels may also show x-ray findings of resporption, fragmentation and increased density. But they occur much less often in the normal foot. Pulling or ?traction? of the Achilles tendon on the unossified growth plate is a likely contributing factor to Sever?s disease. Excessive pronation and a tight Achilles and limited dorsiflexion may also contribute to the development of this condition.
Non Surgical Treatment
Cold packs: Apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking.
Shoe inserts: Small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term.
Medication: Pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor).
Anti-inflammatory creams: Also an effective management tool.
Splinting or casting: In severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare.
Time: Generally the pain will ease in one to two weeks, although there may be flare-ups from time to time.
Correction of any biomechanical issues: A physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition.
Education: Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Foot Arches Pain In Left Side
Overview
Arch pain is felt on the underside of your foot between the heel and ball. The purpose of the arch is to transfer your body weight from heel to toe, and pain is the result when the arch doesn?t function properly. Your foot actually contains two arches: the longitudinal arch which runs the length of your foot, and the transverse arch (also known as the metatarsal arch) which spans the width of your foot. There are 24 bones which create the arches and these bones are held together through their unique interlocking shapes and ligaments. The muscles and the plantar fascia (a broad band of fibrous tissue which runs from the heel to the toes) provide secondary support, and fat pads help to absorb impact and bear your weight. If any of these structures or their interaction are damaged or faulty, arch pain may occur. The most common cause of arch pain is plantar fasciitis, an inflammation of the plantar fascia. You may also suffer arch pain if you have a structural imbalance in your foot or suffer from arthritis. But arch pain may also result from stepping on a rock or when someone steps on your foot. This force may cause an injury such as a bone fracture or damage to the supporting muscles, ligaments, or tendons underneath your foot.

Causes
In most cases, plantar fasciitis develops without a specific, identifiable reason. There are, however, many factors that can make you more prone to the condition. Tighter calf muscles that make it difficult to flex your foot and bring your toes up toward your shin. Obesity. Very high arch. Repetitive impact activity (running/sports). New or increased activity.Although many people with plantar fasciitis have heel spurs, spurs are not the cause of plantar fasciitis pain. One out of 10 people has heel spurs, but only 1 out of 20 people (5%) with heel spurs has foot pain. Because the spur is not the cause of plantar fasciitis, the pain can be treated without removing the spur.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused.
Diagnosis
To come to a correct diagnosis, your podiatrist will examine your foot by using his or her fingers to look for a lump or stone bruise in the ball of your foot. He or she will examine your foot to look for deformities such as high or low arches, or to see if you have hammertoes. He or she may use x-rays, MRIs (magnetic resource imaging), and CT scans to rule out fractures and damage to ligaments, tendons, and other surrounding tissues. Your doctor will also inquire about your daily activities, symptoms, medical history, and family history. If you spend a lot of time running or jumping, you may be at a higher risk for pain in the bottom of your foot. These diagnostic tests will help your doctor come to a proper diagnosis and create an appropriate treatment plan.
Non Surgical Treatment
Stretch the fascia. Prop your toes up against a wall, keeping your arch and heel flat so the toes stretch. Hold for a count of 10. Repeat 10 times three or four times per day. Roll a frozen water bottle under the arch. Stretch first then roll out the arch for 10 minutes; you don?t want to stretch the tendon when it?s ice cold. Freeze a golf ball and massage the fascia. Roll the frozen golf ball under the foot, starting from the front and working your way back. Put good pressure on each spot-the medial, center and lateral positions-for 15 seconds before moving to the next area. Then, roll the ball back and forth over the entire foot. Foam roll all muscles on the body above the plantar. Even tight shoulders can cause the condition, as your arm swing can throw off proper hip alignment and footstrike. Bump your arch. Get a commercial insole with an arch bump to push on the plantar and keep it from flexing-it doesn?t matter if you?re an under or overpronator; the plantar needs to be supported and strengthened, Wear the support in all shoes, if possible.
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions.
Prevention
People who run regularly should replace shoes every six months, more frequently if an avid runner. Avoid running or stepping on uneven surfaces. Try to be careful on rocky terrain or hills with loose gravel. Holes, tree stumps and roots are problems if you are trail running. If you have problems with the lower legs, a dirt road is softer than asphalt, which is softer than concrete. Try to pick a good surface if possible. However, if you're racing, be sure to train on the surface you'll eventually run on. Be careful running too many hills. Running uphill is a great workout, but make sure you gradually build this up to avoid injuries. Be careful when running downhill too fast, which can often lead to more injuries than running uphills. Prevent recurrent injuries. Athletes who have experienced ankle injuries previously may benefit from using a brace or tape to prevent recurrent ankle injuries.
Arch pain is felt on the underside of your foot between the heel and ball. The purpose of the arch is to transfer your body weight from heel to toe, and pain is the result when the arch doesn?t function properly. Your foot actually contains two arches: the longitudinal arch which runs the length of your foot, and the transverse arch (also known as the metatarsal arch) which spans the width of your foot. There are 24 bones which create the arches and these bones are held together through their unique interlocking shapes and ligaments. The muscles and the plantar fascia (a broad band of fibrous tissue which runs from the heel to the toes) provide secondary support, and fat pads help to absorb impact and bear your weight. If any of these structures or their interaction are damaged or faulty, arch pain may occur. The most common cause of arch pain is plantar fasciitis, an inflammation of the plantar fascia. You may also suffer arch pain if you have a structural imbalance in your foot or suffer from arthritis. But arch pain may also result from stepping on a rock or when someone steps on your foot. This force may cause an injury such as a bone fracture or damage to the supporting muscles, ligaments, or tendons underneath your foot.
Causes
In most cases, plantar fasciitis develops without a specific, identifiable reason. There are, however, many factors that can make you more prone to the condition. Tighter calf muscles that make it difficult to flex your foot and bring your toes up toward your shin. Obesity. Very high arch. Repetitive impact activity (running/sports). New or increased activity.Although many people with plantar fasciitis have heel spurs, spurs are not the cause of plantar fasciitis pain. One out of 10 people has heel spurs, but only 1 out of 20 people (5%) with heel spurs has foot pain. Because the spur is not the cause of plantar fasciitis, the pain can be treated without removing the spur.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused.
Diagnosis
To come to a correct diagnosis, your podiatrist will examine your foot by using his or her fingers to look for a lump or stone bruise in the ball of your foot. He or she will examine your foot to look for deformities such as high or low arches, or to see if you have hammertoes. He or she may use x-rays, MRIs (magnetic resource imaging), and CT scans to rule out fractures and damage to ligaments, tendons, and other surrounding tissues. Your doctor will also inquire about your daily activities, symptoms, medical history, and family history. If you spend a lot of time running or jumping, you may be at a higher risk for pain in the bottom of your foot. These diagnostic tests will help your doctor come to a proper diagnosis and create an appropriate treatment plan.
Non Surgical Treatment
Stretch the fascia. Prop your toes up against a wall, keeping your arch and heel flat so the toes stretch. Hold for a count of 10. Repeat 10 times three or four times per day. Roll a frozen water bottle under the arch. Stretch first then roll out the arch for 10 minutes; you don?t want to stretch the tendon when it?s ice cold. Freeze a golf ball and massage the fascia. Roll the frozen golf ball under the foot, starting from the front and working your way back. Put good pressure on each spot-the medial, center and lateral positions-for 15 seconds before moving to the next area. Then, roll the ball back and forth over the entire foot. Foam roll all muscles on the body above the plantar. Even tight shoulders can cause the condition, as your arm swing can throw off proper hip alignment and footstrike. Bump your arch. Get a commercial insole with an arch bump to push on the plantar and keep it from flexing-it doesn?t matter if you?re an under or overpronator; the plantar needs to be supported and strengthened, Wear the support in all shoes, if possible.
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions.
Prevention
People who run regularly should replace shoes every six months, more frequently if an avid runner. Avoid running or stepping on uneven surfaces. Try to be careful on rocky terrain or hills with loose gravel. Holes, tree stumps and roots are problems if you are trail running. If you have problems with the lower legs, a dirt road is softer than asphalt, which is softer than concrete. Try to pick a good surface if possible. However, if you're racing, be sure to train on the surface you'll eventually run on. Be careful running too many hills. Running uphill is a great workout, but make sure you gradually build this up to avoid injuries. Be careful when running downhill too fast, which can often lead to more injuries than running uphills. Prevent recurrent injuries. Athletes who have experienced ankle injuries previously may benefit from using a brace or tape to prevent recurrent ankle injuries.
Acquired Flat Foot Deformity Correction
Overview
Adult-acquired flatfoot (AAF) is the term used to describe the progressive deformity of the foot and ankle that, in its later stages, results in collapsed and badly deformed feet. Although the condition has been described and written about since the 1980s, AAF is not a widely used acronym within the O&P community-even though orthotists and pedorthists easily recognize the signs of the condition because they treat them on an almost daily basis. AAF is caused by a loss of the dynamic and static support structures of the medial longitudinal arch, resulting in an incrementally worsening planovalgus deformity associated with posterior tibial (PT) tendinitis. Over the past 30 years, researchers have attempted to understand and explain the gradual yet significant deterioration that can occur in foot structure, which ultimately leads to painful and debilitating conditions-a progression that is currently classified into four stages. What begins as a predisposition to flatfoot can progress to a collapsed arch, and then to the more severe posterior tibial tendon dysfunction (PTTD). Left untreated, the PT tendon can rupture, and the patient may then require a rigid AFO or an arthrodesis fixation surgery to stabilize the foot in order to remain capable of walking pain free. 
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
Symptoms shift around a bit, depending on what stage of PTTD you?re in. For instance, you?re likely to start off with tendonitis, or inflammation of the posterior tibial tendon. This will make the area around the inside of your ankle and possibly into your arch swollen, reddened, warm to the touch, and painful. Inflammation may actually last throughout the stages of PTTD. The ankle will also begin to roll towards the inside of the foot (pronate), your heel may tilt, and you may experience some pain in your leg (e.g. shin splints). As the condition progresses, the toes and foot begin to turn outward, so that when you look at your foot from the back (or have a friend look for you, because-hey-that can be kind of a difficult maneuver to pull off) more toes than usual will be visible on the outside (i.e. the side with the pinky toe). At this stage, the foot?s still going to be flexible, although it will likely have flattened somewhat due to the lack of support from the posterior tibial tendon. You may also find it difficult to stand on your toes. Finally, you may reach a stage in which your feet are inflexibly flat. At this point, you may experience pain below your ankle on the outside of your foot, and you might even develop arthritis in the ankle.
Diagnosis
Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. 
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
The Causes And Treatment
Overview
Collapsed arches occur in five percent of adults 40 years and older, especially those who are overweight or maintain sedentary lifestyles. At the onset of the condition, adult acquired flatfoot can be controlled with anti-inflammatory medications, physical therapy, taping, bracing, and orthotics. While most cases of adult-onset flatfoot require surgery, congenital flatfoot is an entirely different condition that is best treated with orthotics in children. Ninety percent of children born with flat feet will be fine with conservative treatment. 
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
PTTD begins with a gradual stretching and loss of strength of the posterior tibial tendon which is the most important tendon supporting the arch of the human foot. Left untreated, this tendon will continue to lengthen and eventually rupture, leading to a progressive visible collapse of the arch of the foot. In the early stages, patients with PTTD will notice a pain and swelling along the inner ankle and arch. Many times, they are diagnosed with ?tendonitis? of the inner ankle. If the foot and ankle are not properly supported during this early phase, the posterior tibial tendon can rupture and devastating consequences will occur to the foot and ankle structure. The progressive adult acquired flatfoot deformity will cause the heel to roll inward in a ?valgus? or pronated direction while the forefoot will rotate outward causing a ?duckfooted? walking pattern. Eventually, significant arthritis can occur in the joints of the foot, the ankle and even the knee. Early diagnosis and treatment is critical so if you have noticed that one, or both, of your feet has become flatter in recent times come in and have it checked out.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
Treatment will vary depending on the degree of your symptoms. Generally, we would use a combination of rest, immobilization, orthotics, braces, and physical therapy to start. The goal is to keep swelling and inflammation under control and limit the stress on the tendon while it heals. Avoidance of activities that stress the tendon will be necessary. Once the tendon heals and you resume activity, physical therapy will further strengthen the injured tendon and help restore flexibility. Surgery may be necessary if the tendon is torn or does not respond to these conservative treatment methods. Your posterior tibial tendon is vital for normal walking. When it is injured in any way, you risk losing independence and mobility. Keep your foot health a top priority and address any pain or problems quickly. Even minor symptoms could progress into chronic problems, so don?t ignore your foot pain. .jpg)
Surgical Treatment
If surgery is necessary, a number of different procedures may be considered. The specifics of the planned surgery depend upon the stage of the disorder and the patient?s specific goals. Procedures may include ligament and muscle lengthening, removal of the inflamed tendon lining, tendon transfers, cutting and realigning bones, placement of implants to realign the foot and joint fusions. In general, early stage disease may be treated with tendon and ligament (soft-tissue) procedures with the addition of osteotomies to realign the foot. Later stage disease with either a rigidly fixed deformity or with arthritis is often treated with fusion procedures. If you are considering surgery, your doctor will speak with about the specifics of the planned procedure.
Acquired Flat Foot Causes
Overview
Adult acquired flatfoot deformity (AAFD), embraces a wide spectrum of deformities. AAFD is a complex pathology consisting both of posterior tibial tendon insufficiency and failure of the capsular and ligamentous structures of the foot. Each patient presents with characteristic deformities across the involved joints, requiring individualized treatment. Early stages may respond well to aggressive conservative management, yet more severe AAFD necessitates prompt surgical therapy to halt the progression of the disease to stages requiring more complex procedures. We present the most current diagnostic and therapeutic approaches to AAFD, based on the most pertinent literature and our own experience and investigations. 
Causes
Obesity - Overtime if your body is carrying those extra pounds, you can potentially injure your feet. The extra weight puts pressure on the ligaments that support your feet. Also being over weight can lead to type two diabetes which also can attribute to AAFD. Diabetes - Diabetes can also play a role in Adult Acquired Flatfoot Deformity. Diabetes can cause damage to ligaments, which support your feet and other bones in your body. In addition to damaged ligaments, uncontrolled diabetes can lead to ulcers on your feet. When the arches fall in the feet, the front of the foot is wider, and outer aspects of the foot can start to rub in your shoe wear. Patients with uncontrolled diabetes may not notice or have symptoms of pain due to nerve damage. Diabetic patient don?t see they have a problem, and other complications occur in the feet such as ulcers and wounds. Hypertension - High blood pressure cause arteries narrow overtime, which could decrease blood flow to ligaments. The blood flow to the ligaments is what keeps the foot arches healthy, and supportive. Arthritis - Arthritis can form in an old injury overtime this can lead to flatfeet as well. Arthritis is painful as well which contributes to the increased pain of AAFD. Injury - Injuries are a common reason as well for AAFD. Stress from impact sports. Ligament damage from injury can cause the bones of the foot to fallout of ailment. Overtime the ligaments will tear and result in complete flattening of feet.
Symptoms
Your feet tire easily or become painful with prolonged standing. It's difficult to move your heel or midfoot around, or to stand on your toes. Your foot aches, particularly in the heel or arch area, with swelling along the inner side. Pain in your feet reduces your ability to participate in sports. You've been diagnosed with rheumatoid arthritis; about half of all people with rheumatoid arthritis will develop a progressive flatfoot deformity.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
The following is a summary of conservative treatments for acquired flatfoot. Stage 1, NSAIDs and short-leg walking cast or walker boot for 6-8 weeks; full-length semirigid custom molded orthosis, physical therapy. Stage 2, UCBL orthosis or short articulated ankle orthosis. Stage 3, Molded AFO, double-upright brace, or patellar tendon-bearing brace. Stage 4, Molded AFO, double-upright brace, or patellar tendon-bearing brace. 
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Symptomatic flexible flatfoot conditions are common entities in both the adolescent and adult populations. Ligamentous laxity and equinus play a significant role in most adolescent deformities. Posterior tibial tendon dysfunction (PTTD) is the most common cause of adult acquired flatfoot. One should consider surgical treatment for patients who have failed nonoperative therapy and have advancing symptoms and deformities that significantly interfere with the functional demands of daily life. Isolated Joint Fusion. This technique is used for well reducible flat foot by limiting motion at one or two joints that are usually arthritic. The Evans Anterior Calcaneal Osteotomy. This is indicated for late stage II adult acquired flatfoot and the flexible adolescent flatfoot. This procedure will address midtarsal instability, restore the medial longitudinal arch and reduce mild hind foot valgus. The Posterior Calcaneal Displacement Osteotomy (PCDO). This technique is indicated for late stage I and early stage II PTTD with reducible Calcaneal valgus. This is often combined with a tendon transfer. A PCDO is also indicated as an adjunctive procedure in the surgical reconstruction of the severe flexible adolescent flatfoot. Soft tissue procedure. On their own these are not very effective but in conjunction with an osseous procedure, soft tissue procedures can produce good outcome. Common ones are tendon and capsular repair, tendon lengthening and transfer procedures. Flat foot correction requires lengthy post operative period and a lot of patience. Your foot may need surgery but you might simply not have the time or endurance to go through the rehab phase of this type of surgery. We will discuss these and type of procedures necessary for your surgery in length before we go further with any type of intervention.